60/M ALTERED SENSORIUM 2°TO ?ACUTE ISCHEMIC STROKE ?MENINGITIS
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centred online learning portfolio and your valuable inputs on the comment box is welcome."I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan
CHEIF COMPLAINTS AND HOPI.
A 60 year old male who is a resident in telangana ,he does a cotton business. Came to the casualty in altered sensorium on 30/04/2023.
Patient was apparently asymptomatic 10 years back then he developed fever and went to a ayurvedic doctor and was found to be having retroviral postive.
And started using herbal medicine for that and the symptoms he was experiencing back then was subsided.
1month back patient developed weakness in his left hand with tingling and numbness sensation which is insidious in onset and gradually progressive in nature with no aggravating and releiving factors for that he visited the same previous Ayurveda doctor and started using some herbal medicine prescribed by him and then, 3to 4 days later, he developed fever (on and off) and no chills and rigors, which is insidious in onset and gradually progressive in nature along with the fever he also started experiencing leg (both the legs)pain and weakness as well as flank pain for which he went to the same Ayurvedic doctor and he got a scan done the doctor told him that he had stones in his kidneys and prescribed some herbal medicine with dolo and multivitamin tablets. But after this also the fever did not subsided so they again went to him (Ayurvedic doc) 10 days back and the doctor adviced some investigations and after that he told that his viral load is high and prescribed herbal medicine which are of high dose and after using this high dose herbal medicine for 4 to 5 days the patient developed dysphagia and pain in the throat which is insidious in onset and gradually progressive in nature (dysphagia initially to solids and then later to liquids).
He also developed cough 4 days back which is insidious in onset and gradually progressive in nature no history of weight loss,no history of night sweats and after that his responsiveness was decreased and now presented with altered sensorium.
PSYCHOSOCIAL HISTORY: This patient has a friendly relationship with his family friends as well as neighbors
PAST HISTORY:
Know case of HIV POSTIVE since 10 years
Known case hypertensive since 3 years.
Not a known case of DM2,ASTHMA,EPILEPSY,TB,CAD.
DAILY ROUTINE:
He does cotton business.
He daily wakes at 5 Am and takes bath and fresh up drinks tea at 7am and then he takes his breakfast (RICE with vegetable curry )at 8am and goes for his business and comes at 1 pm and takes his lunch which consisting of a vegetable curry and rice and after his lich he chit chat with his neighbors and lie down for some time and after that he watch TV and then eats his dinner at 8pm and goes to sleep at 9pm.
Family history:No similar complaints in the family .This old man has 4 childern(2 sons and 2daughters) and his wife died 5 years ago due to some health issues.
PERSONAL HISTORY:
DIET:VEGETERIAN
APPETITE:DECREASED SINCE 2 MONTHS
BOWEL BLADDER :NOT PASSING STOOLS SINCE 4 DAYS.
SLEEP:ADEQUATE
ADDICTIONS:HE STARTED TAKING BEER 15 DAYS BACK FROM THIS ILLNESS FOR 10 DAYS.
GENERAL EXAMINATION:
Patient is drowsy but arousal.
GCS:E2V1M5
BP:130/80mmhg.
PR:110/min
RR:18CPM
SPO2:95%ON 8 LIT OF O2
TEMP: 99°F
PALLOR PRESENT,no icterus,cyanosis,clubbing,lymphadenopathy and edema
SYSTEMIC EXAMINATION:
CVS:S1,S2 HEARD,NO MURMURS.
RS:BAE+,NVBS.
PA:SOFT AND NONTENDER
CNS:PUPILS :NORMAL SIZE AND NON REACTIVE.
TONE: RT. LT
UL HYPER. HYPER
LL HYPER. NORMAL
POWER:
UL 2/5. 2/5
LL 2/5. 2/5
REFLEXES:
B: 3+ 3+
T: 2+ 2+
S: 2+ 2+
K: 2+ 3+
A: 1+ 1+
P: EXTENSORS
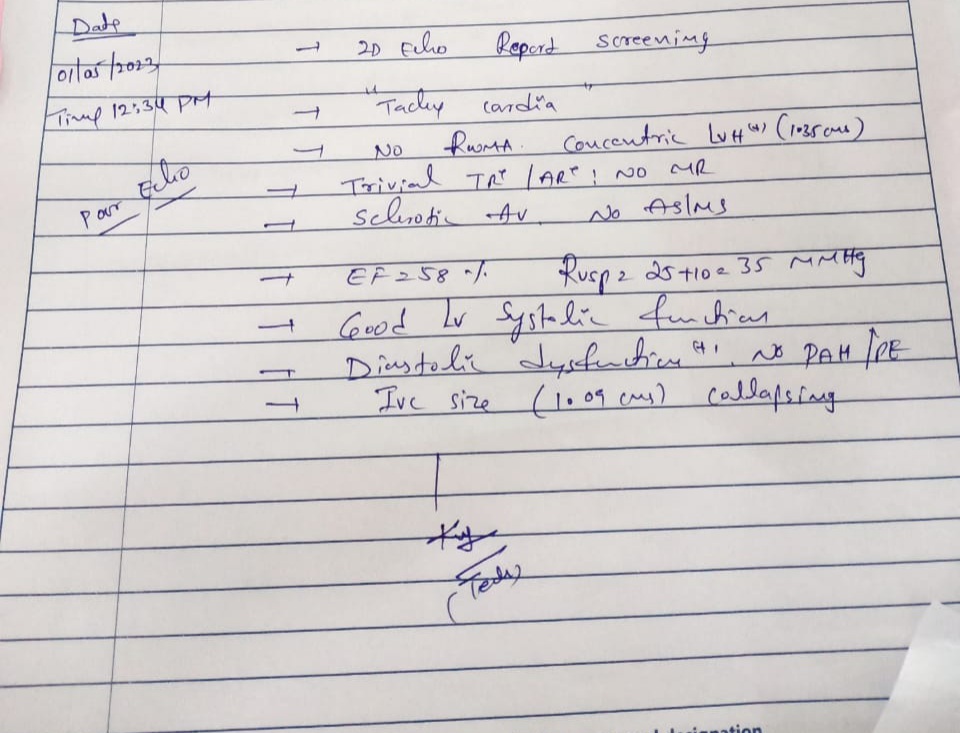
CLINICAL IMAGES AND INVESTIGATIONS
30/04/23














































.jpg)




S:
5 FEVER SPIKES SINCE YESTERDAY 8AM
STOOLS NOT PASSED .
O:
On examination
Patient is drowsy but arousal.
GCS:E1V1M3
BP:110/80mmhg.
PR:140/min
RR:22CPM
SPO2:95%ON 8 LIT OF O2
TEMP: 98°F
CVS:S1,S2 HEARD,NO MURMURS.
RS:BAE+,NVBS.
PA:SOFT AND NONTENDER
CNS:PUPILS :DOLLS EYE+
PUPILS NORMAL SIZE AND NON REACTIVE TO LIGHT.
TONE: RT. LT
UL HYPER. HYPER
LL HYPER. HYPER
POWER:
UL 2/5. 0/5
LL 2/5. 0/5
REFLEXES:
B: 2+ 2+
T: 2+ 2+
S: 2+ 2+
K: 2+ 3+
A: 1+ 1+
P: EXTENSORS
A:
ALTERED SENSORIUM 2°TO ?MENINGITIS,2°TO ?TB,?ACUTE ISCHEMIC STROKE. RETROVIRAL POSTIVE (10 YEARS)WITH KNOWN HYPERTENSIVE SINCE 3 YEARS .
P:
RYLES FEEDING :100ML OF WATER EVERY 2ND HOURLY.
200ML OF MILK EVERY 4TH HOURLY.
IVF:NS@75ml/hr.
Inj.NEOMOL. 1gram IV/SOS. IF TEMP IS greater than 101°F.
SUCTION 2ND HOURLY.
MONITORING VITALS HOURLY
S:
3 FEVER SPIKES SINCE YESTERDAY 8AM( at 4pm,5pm,10pm)
STOOLS NOT PASSED .
O:
On examination
Patient is drowsy but arousal.
GCS:E2V2M3
BP:130/90mmhg.
PR:98/min
RR:26CPM
SPO2:96%ON 8 LIT OF O2
TEMP: 98°F
CVS:S1,S2 HEARD,NO MURMURS.
RS:BAE+,NVBS.
PA:SOFT AND NONTENDER
CNS:PUPILS :DOLLS EYE+
PUPILS NORMAL SIZE AND NON REACTIVE TO LIGHT.
TONE: RT. LT
UL HYPER. HYPER
LL HYPER. HYPER
POWER:
UL 2/5. 0/5
LL 2/5. 0/5
REFLEXES:
B: 1+ 1+
T: 1+ 1+
S: 1+ 1+
K: 1+ 1+
A: 1+ 1+
P: EXTENSORS
A:
ALTERED SENSORIUM 2°TO ? TB MENINGITIS,RETROVIRAL POSTIVE (10 YEARS)WITH KNOWN HYPERTENSIVE SINCE 3 YEARS .
P:
RYLES FEEDING :100ML OF WATER EVERY 2ND HOURLY.
200ML OF MILK EVERY 4TH HOURLY.
IVF:NS@75ml/hr.
Inj.NEOMOL. 1gram IV/SOS. IF TEMP IS greater than 101°F.
TAB:ISONIAZID 5mg/kg.PO/OD
Tab:RIFAMPICIN 10mg/kgPO/OD
TAB;PYRAZINAMIDE 25mg/kgPO/OD
TAB:ETHAMBUTOL 15mg/kg PO/OD
TAB:BENADON 40mg po/OD
INJ:DEXA 6mg iv/tid
Inj:PANTOP 40mg iv
SUCTION 2ND HOURLY.
MONITORING VITALS HOURLY.









ICU BED 4 60/M
DR.RAKESH BISWAS(HOD)
DR.ABHINAYA (SR)
DR.NARSIMHA(PGY2)
DR.HIMAJA(PGY1)
DR.KIRAN(PGY1)
S:
3 FEVER SPIKES SINCE YESTERDAY 8AM( at 2AM,3AM,4AM)
STOOLS NOT PASSED .
O:
On examination
Patient is drowsy but arousal.
GCS:E2V2M3
BP:130/80mmhg.
PR:98/min
RR:28CPM
SPO2:96%ON 8 LIT OF O2
TEMP: 98.7°F
CVS:S1,S2 HEARD,NO MURMURS.
RS:BAE+,DECREASED BREATH SOUNDS ON RIGHT SIDE AND BILATERAL GRUNTING PRESENT.
PA:SOFT AND NONTENDER
CNS:PUPILS :DOLLS EYE+
PUPILS NORMAL SIZE AND NON REACTIVE TO LIGHT.
TONE: RT. LT
UL HYPER. HYPER
LL HYPER. HYPER
POWER:
UL 2/5. 2/5
LL 1/5. 1/5
REFLEXES:
B: 2+ 2+
T: 2+ 2+
S: 1+ 1+
K: 2+ 2+
A: 1+ 1+
P: EXTENSORS
A:
ALTERED SENSORIUM 2°TO ? TB MENINGITIS ?FUNGAL MENINGITIS,RETROVIRAL POSTIVE (10 YEARS)WITH KNOWN CASE OF HYPERTENSIVE SINCE 1YEAR WITH GRADE 2 BED SORE.
P:
RYLES FEEDING :100ML OF WATER EVERY 2ND HOURLY.
200ML OF MILK EVERY 4TH HOURLY.
IVF:NS@75ml/hr.
Inj.NEOMOL. 1gram IV/SOS. IF TEMP IS greater than 101°F.
TAB:ISONIAZID 275mg/.PO/OD
Tab:RIFAMPICIN 550mg/PO/OD
TAB;PYRAZINAMIDE 1375mg/PO/OD
TAB:ETHAMBUTOL 825mg/kg PO/OD
TAB:BENADON 40mg po/OD
INJ.FLUCONAZOLE 200MG IV/BD.
INJ:DEXA 6mg iv/tid
Inj:PAN 40mg iv /OD.
SYP.LACTULOSE 15 ml PO/HS.
MUCOMIST NEBULISATION 6TH HOURLY.
NEOSPORIN POWDER FOR L/A AT BED SORE.












Comments
Post a Comment